Expert Stroke Treatment at Affordable Costs
- Stroke-Ready 24/7
- Expertise in Ischemic and Haemorrhagic Strokes
- Dedicated Stroke ICU
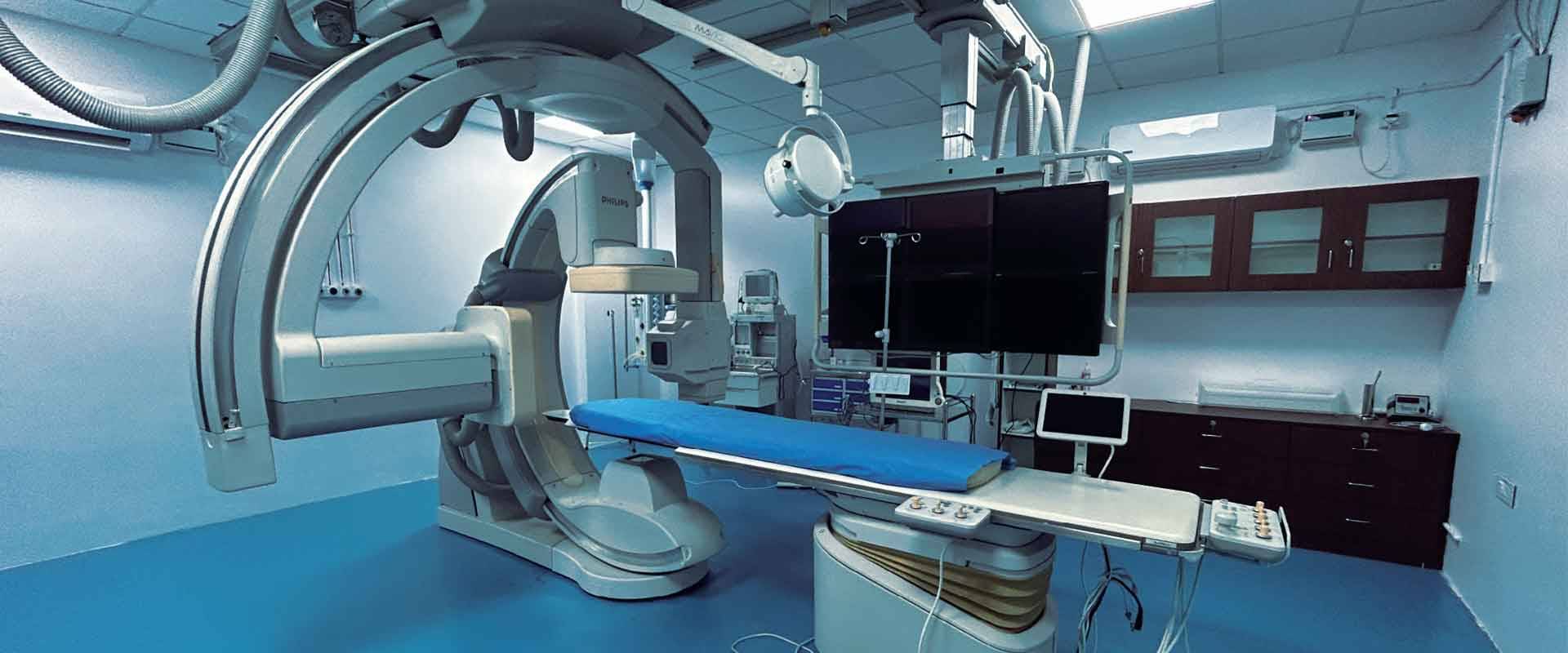
- State-Of-The-Art Biplane Neuro Cath Lab
- Personalised Care
- Pocket-Friendly Costs
Stroke Emergency & Stroke Recovery Specialist
A stroke is a medical emergency that happens when there is a blood flow problem to the brain. Without proper blood supply, brain cells in the affected area begin to die because they don’t receive enough oxygen and nutrients. This damage can lead to a variety of problems, such as difficulty speaking, paralysis, or even life-threatening complications. While you read about it, do keep in mind that at Vanchilingam Advanced Neurology and Stroke we are ready 24/7 to provide the best stroke treatment.

There are two main types of strokes:
- Ischemic Stroke: This is the most common type, occurring when a blood clot or plaque blocks an artery leading to the brain.
- Haemorrhagic Stroke: This occurs when a blood vessel in the brain bursts, causing bleeding and pressure on the brain tissue.
Another condition, known as a Transient Ischemic Attack (TIA) or “mini-stroke,” is a temporary blockage of blood flow to the brain. Although the symptoms resolve within minutes or hours, it serves as a warning sign for a potential major stroke in the future.
The symptoms of a stroke often come on suddenly and may include:
- Weakness or numbness on one side of the body, particularly in the face, arm, or leg.
- Difficulty speaking or understanding speech.
- Blurred or double vision.
- Dizziness, loss of balance, or coordination.
- A sudden, severe headache with no known cause.
When it comes to stroke, time is crucial. The faster you recognize the signs and get help, the better the chances of recovery. Ideally it would be beneficial if help can be called for within 6 to 12 hours after the onset. To identify signs of a stroke just remember the acronym,
BE FAST
Specialized Treatments for Stroke: What We Offer
At Vanchilingam Advanced Neurology and Stroke, we are committed to saving lives and minimizing the impact of stroke through advanced treatments. Our approach is evidence based and depends on the type and severity of the stroke.
Ischemic Stroke Treatment
- Mechanical Thrombectomy: For severe ischemic strokes, a minimally invasive procedure is used to remove the clot. Our expert Interventional Neuroradiologists / Neurologists utilise the Biplane Neuro Cath lab to remove the blocks. This is the gold standard in stroke treatment today.
- Clot-Busting Medications (Thrombolysis): Intravenous tissue plasminogen activator (tPA) is a medication that can dissolve the clot and restore blood flow. This treatment is most effective when administered within 3-4.5 hours of onset of the symptom.
Hemorrhagic Stroke Treatments
- Emergency Surgery: If bleeding occurs in the brain, surgical procedures such as clipping or coiling are performed to stop the bleeding and relieve pressure.
- Medications: Drugs to control blood pressure, prevent seizures, and reduce brain swelling are crucial in managing haemorrhagic strokes.
At Vanchilingam Hospital, we also focus on preventive care, offering:
- Comprehensive stroke risk assessments.
- Blood pressure and cholesterol management.
- Lifestyle counseling for smoking cessation, weight management, and diabetes control.
Why Choose Vanchilingam Hospital for Stroke Care?
When it comes to treating stroke, expertise can make all the difference. For instance, there is no time window for Ischemic Stroke treatment. Mechanical thrombectomy and clot busting drugs can be given up to 24 hours in selected patients. Conventional treatment at other centres stops at 4.5 hours, but due to our vast experience and specialised imaging sequences we can give these treatments at extended time windows.
For Haemorrhagic Stroke, we use an activated Factor VII drug to reduce the expansion of the bleed on a case to case. When used correctly, it reduces mortality and the need for surgery in Haemorrhagic stroke patients.
As a stroke-ready center we pride ourselves on the unparalleled services that we bring to the table:
24/7 Stroke Care Team
Our dedicated stroke care team, including Neurologists, and interventional Neuroradiologists / Neurologists, are available round the clock. This ensures that patients receive prompt and effective care the moment they arrive.
Dedicated Neurocritical Care with Stroke ICU
The Acute Stroke Unit is the acute neurological ward providing specialist services for people who have had a new suspected stroke.
State-of-the-Art Technology
From advanced imaging tools like CT and MRI to cutting-edge intervention equipment, our center is equipped to handle even the most complex stroke cases with precision.
Personalized Care
Every stroke case is unique, and our approach reflects that. We develop tailored treatment plans to maximize recovery potential.
Proven Track Record
Vanchilingam has the credit of having treated over a million patients over the years in every Neurological condition. With a strong history of successful stroke outcomes. Our patients consistently report high satisfaction rates, thanks to our compassionate care, commitment to excellence, all of which come at highly affordable costs.
Choose Vanchilingam Hospital: Your Partner in Stroke Recovery
A stroke can be life-changing, but with the right care and timely intervention, recovery is possible. At Vanchilingam, we combine expertise, advanced technology, and compassionate care to ensure the best outcomes for our patients. Whether it’s emergency treatment, rehabilitation, or preventive care, we are here to support you and your loved ones every step of the way.
Don’t wait when it comes to stroke. If you or someone you know is experiencing symptoms, act fast and trust Vanchilingam Advanced Neurology and Stroke for expert care.
For more information or to schedule a consultation, contact us today.
Meet the Specialists
Our team of dedicated specialists brings years of expertise and a passion for delivering personalized care.








Real Experiences, Real Results
Discover how Dr. Vanchilingam Advanced Neuro & Stroke Hospital has transformed the lives of our patients. Also hear our specialists talk about the services and solutions we offer for various neurological issues.



OUR SPECIALITY
Acute Stroke Unit
The Acute Stroke Unit is an acute neurological ward providing specialist services for people who have had a new suspected stroke. On the Acute Stroke Unit we provide: Thrombolysis treatment -treatment is started in the Emergency Department and you will have the rest of your Treatment and monitoring on the Acute Stroke Unit
OUR SPECIALITY
Advanced Neuro ICU
A neuro ICU is an Intensive Care Unit which is particularly devoted to a high – quality care of patients with the neurological problems that are life-threatening in nature. The neuro ICU of our hospital is a complete state of the art and a full-fledged one designed to provide almost all sorts of advanced neurological care to the normal patients as well as the patients in the emergency.
OUR SPECIALITY
Advanced Neuro Imaging
Our radiology department is a state of the art department with all the necessary infrastructure that is essential for effectively dealing with the neuro and neurosurgery emergencies at its best. The advanced neuroimaging techniques used by our doctors are as discussed below.
OUR SPECIALITY
Neuro interventional Cath Lab
A neuro-interventional Cath lab in a neurodiagnostic Centre is a specialized catheterization laboratory which has all the necessary diagnostic imaging equipment that is particularly used for the purpose of visualization of the arteries, veins and other vascular malformations of the brain and spinal cord.
OUR SPECIALITY
Neuro-Surgery Operating Room
The neurosurgery operating room of Dr.Vanchilingam Hospital, Neurosurgery Hospital is a fully functional and a state of art one that has the adequate infrastructure for effectively carrying out even the most complicated neuro surgeries with ease.
What is a stroke, and why is it a medical emergency?
A stroke occurs when the blood flow to the brain is interrupted, depriving brain cells of oxygen and nutrients. This can lead to severe complications, including difficulty speaking, paralysis, or life-threatening conditions. Immediate medical attention is crucial for minimizing damage and improving recovery outcomes.
What are the different types of strokes?
There are three main types of strokes:
- Ischemic Stroke: Caused by a blood clot or plaque blocking an artery in the brain.
- Haemorrhagic Stroke: Occurs when a blood vessel bursts, causing bleeding in the brain.
- Transient Ischemic Attack (TIA): A temporary blockage often called a “mini-stroke,” which serves as a warning for future major strokes.
What are the common symptoms of a stroke?
Stroke symptoms often come on suddenly and may include:
- Weakness or numbness on one side of the body, particularly in the face, arm, or leg.
- Difficulty speaking or understanding speech.
- Vision problems such as blurred or double vision.
- Sudden dizziness or loss of balance.
- Severe headache with no known cause.
How can I quickly identify a stroke?
Use the acronym BE FAST:
Balance: Sudden loss of balance or coordination.
Eyes: Trouble seeing in one or both eyes.
Face: Facial drooping on one side.
Arms: Weakness or numbness in one arm.
Speech: Slurred or confused speech.
Time: Call emergency services immediately.
What stroke treatments are available at Vanchilingam Advanced Neurology and Stroke?
We offer advanced treatments tailored to the type of stroke:
- Ischemic Stroke: Mechanical thrombectomy and clot-busting medications like tPA.
- Haemorrhagic Stroke: Emergency surgeries and medications to control bleeding and reduce brain swelling.
What makes Vanchilingam Advanced Neurology and Stroke unique in stroke care?
Our hospital specializes in:
- Treating ischemic strokes up to 24 hours after onset in select patients.
- Using advanced imaging and Factor VII medication for haemorrhagic strokes.
- Providing 24/7 care with a dedicated Stroke ICU and advanced technology like the Biplane Neuro Cath Lab.
How does Vanchilingam Hospital support stroke recovery and rehabilitation?
We offer personalized rehabilitation plans, including physical therapy, speech therapy, and counselling. Our team works closely with patients to maximize recovery and improve their quality of life.
Can strokes be prevented?
Yes, preventive care includes:
- Managing risk factors like high blood pressure, high cholesterol, and diabetes.
- Adopting a healthy lifestyle with regular exercise, a balanced diet, and quitting smoking.
- Undergoing regular stroke risk assessments.
What is the time window for stroke treatment?
Time is critical in stroke treatment. Treatments like thrombolysis are most effective within 3-4.5 hours, but advanced options at Vanchilingam Advanced Neurology and stroke extend care for ischemic strokes up to 24 hours in eligible cases.
Why choose Vanchilingam Hospital for stroke care?
With over a million successful neurological cases treated, we combine expertise, state-of-the-art technology, and compassionate care at pocket-friendly costs. Our proven track record ensures the best outcomes for stroke patients.